





According to a Bloomberg report written by Stephanie Baker, the University of Oxford candidate, led by Sarah Gilbert, might be through human trials in September. AstraZeneca has lined up agreements to produce 2 billion doses.
This might be the potential COVID19 vaccine that we have been looking for. Research data from the phase 1 trials are scheduled to be declared today

How Did it Unfold?
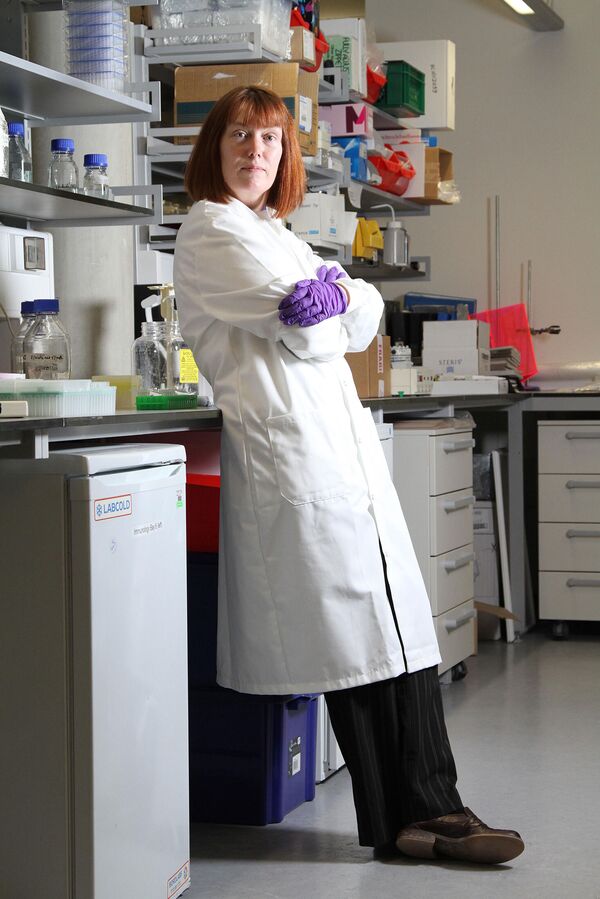
It was their mother’s vaccine—she leads the University of Oxford team that developed it—but there wasn’t a big family talk. “We didn’t really discuss it as I wasn’t home much at the time,” Gilbert told me recently. She’d been working around the clock, as one does while trying to end a pandemic, and at any rate wasn’t worried for her kids. “We know the adverse event profile and we know the dose to use, because we’ve done this so many times before,” she says. “Obviously we’re doing safety testing, but we’re not concerned.”
Determining the Vaccine Efficacy
- In April, Oxford struck a deal with British pharmaceutical giant AstraZeneca Plc to spearhead global manufacturing and distribution and help run more trials around the world.
- AstraZeneca has agreed to sell the vaccine on a not-for-profit basis during the crisis if it proves effective and has lined up deals with multiple manufacturers to produce more than 2 billion doses.
The Life of a Scientist
Gilbert has been all over the British press, but she appears to regard public attention as a distraction. For more than two decades she worked anonymously, developing vaccines while also, of necessity, churning out endless grant applications. Her research was rarely discussed outside scientific circles. Now she’s leading one of the most high-profile and advanced vaccine candidates against Covid-19, with Phase III, or final-stage, trials under way involving thousands of people in Brazil, South Africa, the U.K., and, soon, the U.S. Money is no longer a struggle.
Read More: 90% Effective Oxford Vaccine, Yet To Confirm COVID19 Prevention Capacity
Beginning of Human Trials
At the end of April, crunching a process that normally takes about five years into less than four months, Gilbert and her colleagues at Oxford’s Jenner Institute started a human trial on 1,100 people.
- When Gilbert testified before a parliamentary committee in early July, one member compared her effort to going into a shed and coming out with a jet engine.
- Gilbert’s team has leapfrogged other vaccine contenders to the point where it will likely finish vaccinating subjects in its big 10,000-person efficacy trial before other candidates even start testing on that scale, Kate Bingham, chair of the U.K. government’s Vaccine Taskforce, told the parliamentary committee in early July.
“She’s well ahead of the world,” Bingham said. “It’s the most advanced vaccine anywhere.”

Note of Caution from Peers
Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases (NIAID), has sounded a note of caution about Oxford’s front-runner status. “You’ve got to be careful if you’re temporarily leading the way vs. having a vaccine that’s actually going to work,” he told the BBC recently. Most vaccines in development fail to get licensed. Unlike drugs to treat diseases, vaccines are given to healthy people to prevent illness, which means regulators set a high bar for approval and usually want to see years’ worth of safety data. In the Covid-19 pandemic, it’s not yet clear what regulators will accept as proof of a successful and safe vaccine.
The U.S. Food and Drug Administration has said a vaccine would need to be 50% more effective than a placebo to be approved and would need to show more evidence than blood tests indicating an immune response.
Regulators in other countries haven’t spelled out what would be acceptable.
Confident of Vaccine Breakthrough
Gilbert has voiced remarkable confidence in her chances, saying the Oxford vaccine has an 80% probability of being effective in stopping people who are exposed to the novel coronavirus from developing Covid-19. She has said she could know by September.
Asked by MPs in early July whether the world would have to struggle through the winter without a vaccine, Gilbert said, “I hope we can improve on those timelines and come to your rescue.”
Gilbert, who is 58, has the hyperefficient, serious demeanor you’d expect from someone who might be on the cusp of a breakthrough and hasn’t a minute to spare. When I first called her in early March, she abruptly ended the conversation after 10 minutes to speak to someone about the technical process of manufacturing the vaccine. It would have been crazy to take offense.
Gilbert says she wakes up at around 4 a.m. most days “with lots of questions in my head,” works from home for a few hours, then rides her bicycle to the institute, where she works into the evening. The Oxford team, just a handful of people in January, now comprises roughly 250.
How the Vaccine Works?
The vaccine is a so-called viral vector type based on years of research by Gilbert and Adrian Hill, the head of the Jenner Institute. Traditional vaccines are made with a weakened or inactivated form of the germ that causes infection to stimulate an immune response. Those vaccines aren’t easy to develop and produce quickly.
The Oxford team has developed a technology that can speed up the process by using a harmless virus as a kind of Trojan horse to carry the genetic material of a pathogen into cells to generate an immune response.
- In the case of Covid-19, Gilbert has taken a chimpanzee adenovirus (a common cold virus) and inserted genetic material from the surface spike protein of the SARS-CoV-2 virus as a way of tricking the immune system to fight back.
- The chimp adenovirus platform stimulates both antibodies and high levels of killer T-cells, a type of white blood cell that helps the immune system destroy infection.

Similar To Chinese Efforts
Gilbert’s approach is similar to a viral vector vaccine developed by the Chinese company CanSino Biologics Inc. That one is in Phase II human trials.
The difference between the two is small but may be crucial: CanSino uses a vector based on a human adenovirus that many people have already been infected with.
Early tests showed that people with preexisting antibodies to the adenovirus neutralized the vaccine before it could elicit a strong immune response to SARS CoV-2—the Trojan horse is destroyed before the troops can get out. Johnson & Johnson is developing a similar vaccine based on a human adenovirus; it will begin human trials in the second half of July. All these adenovirus-based vaccines have an advantage over other candidates:
They only need to be kept chilled rather than frozen, making them easier to distribute worldwide.
What would a successful vaccine look like?
A successful vaccine likely won’t be 100% effective, no matter who wins the race, and success might have different definitions.
- Not all vaccines produce what’s called sterilizing immunity, in which the body produces neutralizing antibodies that block a virus from getting into cells.
- Some vaccines don’t prevent infection but trigger the immune system to protect against illness.
Jonas Salk’s polio vaccine doesn’t stop infection but prevents the disease that crippled millions. I asked Gilbert what her definition of a successful vaccine would be, but she wouldn’t be drawn out on specifics. “We need a vaccine with a high level of efficacy against disease, which also has a significant impact on virus transmission,” she said.
The Importance of Speed
In the wake of the Ebola outbreak, Gilbert responded to a call from the World Health Organization for researchers to come up with methods to rapidly respond to a clutch of emerging pathogens. It meant having a plan for “Disease X”—that unknown yet inevitable pathogen lurking around the corner. Before Covid-19 presented as the nightmare Disease X scenario, Gilbert began working on Middle East respiratory syndrome, or MERS—another coronavirus that causes pneumonia and had threatened to spark a global health crisis. It first emerged in 2012 in Saudi Arabia, but an outbreak didn’t occur until 2014. MERS is much more deadly than Covid-19, killing about a third of those infected.

Gilbert worked on a MERS vaccine using the chimp adenovirus, in this case fused with the genetic material of the MERS virus. She traveled to Saudi Arabia in November 2015 for a conference with leading vaccinologists, hoping it would result in funding. It didn’t. She and Hill had government grants to develop a number of vaccines, but that could take them only so far, and in 2016 they created a private company called Vaccitech. It went on to raise more than £30 million ($37.8 million) from Google Ventures (now GV), Sequoia Capital China, and Oxford Sciences Innovation, a venture capital fund set up to commercialize scientific research coming out of Oxford. The company holds the rights to several vaccines Gilbert and Hill are developing using the chimp adenovirus platform, including a promising prostate cancer therapy.
The VC funding, along with some government money, helped them fine-tune the viral vector program and push the MERS vaccine into a small safety trial with 24 people in 2018. The subjects were divided into three groups getting low, intermediate, and high doses. The results, published in April 2020, showed the vaccine was safe and produced an immune response that persisted for a year. It produced high levels of T-cells, but only 44% of people receiving the highest dose generated neutralizing antibodies. That raised the question of whether two doses might be needed. The MERS safety study couldn’t prove whether the combination of T-cells and neutralizing antibodies induced by the vaccine worked to prevent disease, because it was too small and took place in the U.K., which has had only a handful of MERS cases since 2012. In December 2019, just a few weeks before the novel coronavirus emerged in Wuhan, China, Gilbert’s team began a second trial for the MERS vaccine in Saudi Arabia, where most of the world’s cases have been reported. Even there, only about 200 cases of MERS are reported annually, so proving the vaccine works could take many months.
The work gave Gilbert a running start when Covid-19 emerged. “The spike protein of MERS shares a 40% to 50% similarity to the spike of SARS-CoV-2,” says Naif Alharbi, a Saudi scientist who studied under Gilbert at Oxford and is running the trials of the MERS vaccine in Riyadh. “We know the chimp adenovirus is safe in humans, and it’s been tested in humans with the MERS spike. Given the similarities, the only question with the Covid-19 vaccine is whether it’s going to be protective or not.”
“The MERS study was absolutely critical,” says Tom Evans, chief scientific officer of Vaccitech. “We could say, ‘OK, we can start tomorrow.’ We don’t have to make 10 different varieties of this. We knew it could be manufactured. We knew it was immunogenic in humans.”
When she first heard about the cases of pneumonia in China over the New Year, Gilbert was unsure how quickly it would spread. “We didn’t know what it was early on,” she says. “I was talking to colleagues thinking, yeah, as soon as the sequence comes out, we’ll make something; we’ll test it in mice; we’ll show what we can do.” As soon as Chinese scientists published the genetic sequence of the novel coronavirus on Jan. 10, Gilbert got to work.
Oxford had an advantage unusual for an academic institution: its own vaccine manufacturing facility, at which it was able to quickly manufacture the shot for the first phase of human trials.
- Gilbert arranged for the next, larger batch to come from Italian pharma company Advent, and persuaded the university to underwrite the contract until she could secure further funding.
- On Feb. 17 her team began injecting mice with the vaccine. To accelerate a process that normally takes months, she was performing several steps at once—testing in animals, applying to regulators for human trials, and talking to manufacturers.
“Her level of knowledge of the detail is extraordinary,” says Andrew McLean, who worked with her for years as an investor and board member at Vaccitech. “It’s very unusual for a scientist to know the practical parts of getting a drug made and be able to talk to manufacturers on a toe-to-toe basis.”
But in early March, Gilbert was still scrounging for money. “If we don’t have the money now, we can’t get the vaccine manufactured now and we can’t get the trials done,” she told me at the time. “We needed the money a month ago.” She got a small grant from the Coalition for Epidemic Preparedness Innovations, or CEPI, a foundation set up in 2017 with funding from the Bill & Melinda Gates Foundation, the governments of Norway and India, and the Wellcome Trust Ltd., a London-based research charity. It was enough to keep them going.
Around this time, there was a debate within the Jenner Institute about whether to go straight into human trials or wait until they got results from a study of their vaccine in nine rhesus monkeys at the Rocky Mountain Laboratories in Montana, part of the NIAID. They knew that in tests for a vaccine against the first SARS virus, which caused an epidemic in Asia in 2002-03, some vaccinated animals became more severely ill after they were challenged with the virus than unvaccinated ones did. The phenomenon is known as antibody dependent enhancement, or ADE. Scientists around the world were worried that might happen again with a SARS-CoV-2 vaccine, and the Oxford team wanted to test it in monkeys to rule it out. But time was of the essence: People were dying from Covid-19, and waiting for the monkey results would mean losing crucial weeks.
“We were doing that monkey experiment for safety and to convince the pessimists that the vaccine was going to be safe after infection,” Hill says. “The big question was, when you have a vaccine available and you have people lined up ready to go, do you wait for the monkey results to vaccinate them?”
They decided to play it safe and wait while pressing ahead with planning the trials, setting up manufacturing, and looking for more money. On March 23, the same day U.K. Prime Minister Boris Johnson ordered the country into lockdown, the government announced a £2.2 million grant to Gilbert’s team to support testing and manufacturing. Her colleague Sandy Douglas got £400,000 to figure out how to ramp up the manufacturing process to a million-dose scale.
Bill Gates Teamed Up
During the search for money, Bill Gates pushed Gilbert and Hill to partner with a big pharmaceutical company, and as a CEPI founder he had leverage. “We went to Oxford and said, you are doing brilliant work,” Gates recalled in a call with reporters in early June. “You really need to team up, and we told them a list of people to go and talk to.”
The Oxford team was initially reluctant, Hill says, because they’d run plenty of trials on their own. “What we struggle against all the time is the perception from funders that we can’t do this,” he says. They held talks with several potential partners, whom he declined to name, asking them two questions: How much can you manufacture, and by when? “They didn’t answer either of those questions no matter how many times we asked,” Hill recalls.
AstraZeneca Deal
AstraZeneca was different. In early April, Mene Pangalos, the company’s head of research and development for biopharmaceuticals, had been hearing positive things about Oxford’s work. Although AstraZeneca isn’t a big player in vaccines—it produces a nasal flu spray vaccine but nothing else—he thought it was worth calling John Bell, an immunologist and professor who directs the university’s medical research strategy, to find out more. “It seemed like they needed a partner,” Pangalos recalls. “I called John up and said, ‘Are you interested in working with us on this? Because we think we can help.’ ”
Pangalos negotiated the partnership agreement with Bell and the rest of the Oxford team in about 10 days through a flurry of Zoom calls, with Gilbert walking everyone through the data. AstraZeneca agreed to be responsible for worldwide distribution and manufacturing.
After the deal was announced at the end of April, big money followed as Pascal Soriot, AstraZeneca’s chief executive officer, pledged to make the vaccine available at only a “few dollars” per dose. The British government gave £65 million to accelerate the work and secure 30 million doses for the U.K. by September as part of a deal to make 100 million in total, with some reserved for developing countries. Days later, AstraZeneca announced a $1.2 billion deal with the U.S. Biomedical Advanced Research and Development Authority (Barda) to develop and produce 300 million doses, one of the largest deals the agency has announced. AstraZeneca will work with the National Institutes of Health to test it in 30,000 people in the U.S., scheduled to start in August. The company later struck a licensing deal with the Serum Institute of India to produce a billion doses for developing and middle-income countries. Because of expected political pressure—any country with a role in the production of a vaccine might act to secure doses for its own people—AstraZeneca is setting up independent supply chains within countries to prevent delays at national borders.

As the AstraZeneca deal was being finalized in mid-April, the results of the monkey study came through from Montana. “It wasn’t promising—it was fantastic,” Hill says. “Not only were the monkeys fine, but as a bonus we saw some protection.” They’d vaccinated six monkeys and then 28 days later exposed them to a massive dose of SARS-CoV-2 via multiple routes—eyes, mouth, nose, and trachea, to expose the lungs. It was much more than a person might encounter on public transportation or even in a Covid ward. After exposure, the animals showed no signs of pneumonia in their lungs. By all indications, they felt fine. Nasal swabs, however, showed they still had the virus, meaning they might be able to infect others. The study’s aim was to determine safety, not efficacy, so the Jenner team was encouraged to see it provided some protection in the face of an overwhelming dose of the virus. The day after the preliminary results came in, a team headed by Andrew Pollard, a colleague of Gilbert’s running the clinical trials, started injecting people.
When the full results of the monkey trials were published in mid-May, critics pounced, seeing the results as weak. William Haseltine, a former professor at Harvard Medical School who spent years researching HIV, wrote a piece in Forbes arguing that the Oxford vaccine looked like it would be only partially protective, because it didn’t generate high levels of neutralizing antibodies, which defend cells against infection.
“What happens when you have a vaccine with people running around with virus spewing out of their nose? Anyone who is not vaccinated or not vaccinated well is going to get infected,” Haseltine told me on a Zoom call. “My guess is the Oxford vaccine isn’t going to be powerful enough for older people, so they will have to boost it up, and boosting it up can have side effects.”
On July 14 the U.S. government released results from the safety trial of another vaccine candidate, from Moderna Inc. The company’s stock rose sharply on news that the vaccine produced neutralizing antibodies in all patients. (It also produced side effects in some.) Moderna’s vaccine, produced using a technique called messenger RNA, will go into late-stage trials by the end of July.

Not A Complete Knockout
Team Oxford-AstraZeneca argues it’s not realistic to expect clear nasal swabs from monkeys after they got a whopping dose straight up their noses. “It doesn’t need to cure you of SARS-CoV-2,” AstraZeneca’s Pangalos says. “I don’t know if we will completely knock out shedding or people being infectious, whether we’re going to cure people completely or whether we will just dampen down the illness. We want a vaccine to stop people from going to hospital and dying. If you can do that, I think people will be pretty happy. Neutralizing antibodies is one of the things you’ll look at, but the T-cell response is going to be important.”
Hill says the same thing: Haseltine’s focus on neutralizing antibodies is misplaced. Scientific debates aside, I was starting to sense a Harvard-Oxford, American-British rivalry playing out. “It’s simpler to measure antibodies. It’s less expensive, people do it all the time. But often the antibodies are a surrogate for the T-cell number,” Hill says. “Nobody knows in SARS, in MERS, and in Covid-19 the relative importance of those two.”
A flurry of recent research has shown that T-cells may play an important role in responses to SARS-CoV-2. But the only way to know the most effective levels, or titres, of antibodies and T-cells is to test the vaccine in people where the virus is circulating. “No one knows how strong the immune response needs to be to achieve protection in people of any age,” Gilbert says. “If we get a strong T-cell response, we don’t need such a high neutralizing antibody titre to achieve protection. The two arms of the immune response work together to give better protection.” The Jenner Institute team is taking blood samples of people in the trials that began in late April and May in the U.K. to measure antibodies and T-cell responses several weeks after vaccination, but blood results can’t prove it will prevent disease. It’s a numbers game: They’re looking for very few cases of Covid-19 in people who’ve received the vaccine, and a significantly higher number in a control group of people who haven’t. “The better the vaccine is, the quicker you get a result, and the smaller number you need,” Hill says. If they reach, say, 20 cases in the control group and 18 among the vaccinated cohort, that’s not a great vaccine, and they would need a lot of cases to show a difference. But if you have 20 in the control group and two among the vaccinated, “you’re home and dry,” he says.

Human Challenge Trials
Of course, a quicker way of figuring out if it works would be to stage human challenge trials like those done with the monkeys. So far no Covid-19 vaccine developers have used challenge trials because of ethical concerns and the lack of an effective treatment for the disease. That hasn’t stopped more than 30,000 people from more than 140 countries from registering to take part in a potential challenge trial through an organization called 1DaySooner.
When I asked Gilbert in April what was worrying her the most, she said it was going to be difficult to prove the vaccine works as the virus waxes and wanes around the world. “In order to determine vaccine efficacy for any novel coronavirus vaccine, the trial has to be set up in the right place at the right time, and that’s very hard to predict,” she said. “It’s why we’re planning to do multiple trials in multiple countries.” In early June, as U.K. cases began to drop, AstraZeneca set up trials of the vaccine in Brazil and South Africa, where the virus is surging.
Producing millions, if not billions, of doses of the vaccine may be the biggest challenge in the history of the pharmaceutical industry. AstraZeneca is signing production agreements with companies worldwide, including Oxford Biomedica Plc, a small gene and cell therapy company a 10-minute drive from the Jenner Institute. Oxford Biomedica has agreed to produce several million doses, with potential to scale up into the tens of millions if it works. James Miskin, the company’s chief technical officer, describes a multistep production process that sounds to my layperson’s ears like a cross between making a sourdough starter and boiling down sap to make maple syrup.
It begins with nurturing a few milliliters of human embryonic kidney cells, kept in a frozen vial that needs to be gradually defrosted. As the cells are fed a sugar solution, they multiply in a controlled atmosphere of oxygen and carbon dioxide. Over the course of a week, the mixture is moved into larger and larger vessels, and eventually into a 200-liter stainless-steel bioreactor. The master seed stock of the vaccine—which contains the adenovirus with the spike protein—is added to this soupy mixture, which is then stirred, purified, concentrated, and filtered down.

Scaling Up
Scaling the process up to get to millions of doses is full of unknowns, says Matthew Duchars, CEO of the U.K. government-funded Vaccines Manufacturing and Innovation Centre (VMIC), which is helping coordinate British manufacturers. I ask him about the sourdough analogy. “It’s like trying to go from making a loaf of sourdough in your kitchen to making 100,000 sourdough pizzas,” he says. “Scale-up of any process is never as simple as you think it will be, especially with biological material.”
At the end of May, Gilbert’s team pressed ahead with more advanced trials on more than 10,000 people in the U.K. after getting the green light from an independent scientific panel that reviewed its progress so far. To be ready to go, the Oxford group had spent months working with Advent, the Italian manufacturer, to produce the vaccine for the large-scale trials. Under the eye of Stefania Di Marco, a biochemist and Advent’s scientific director, Advent staff worked into the evenings and over weekends to produce 13,000 doses of the vaccine, at a time when Italy was the epicenter of the Covid-19 pandemic. With the seed stock, they made 100 liters of unpurified product and reduced it down to about 3 liters of vaccine. On May 4, they’d finally reached the stage where they could start filling glass vials with the vaccine. Di Marco and about 15 people from her team of 25 gathered that evening as the filling began, with some tears and hugging. “We were excited,” she says. “This is precious material.”
Two weeks later, after extensive checks and documentation, the first shipment of the vaccine arrived in Oxford in temperature controlled boxes. At the end of May, Advent’s batch of vaccine started going into people over the age of 55 to find out if there’s a variation in immune responses to the shot in people of different ages.
How the vaccine performs in this much larger and more diverse group, particularly older people, could well determine whether the Oxford vaccine will help end the pandemic, or whether the world must continue to wait.
Did you subscribe to our daily newsletter?
It’s Free! Click here to Subscribe!
Source: Bloomberg












{kind=link}